
Introduction
The resilience of our society, of the entire globe, is being sorely tested by COVID-19. One Concern was founded to help minimize the disruption and loss from natural disasters, and COVID-19 is a disaster that is straining our resilience fabric.
With our expertise and focus on providing tools to help change outcomes, One Concern is uniquely positioned to contribute to the COVID-19 response efforts. Companies, governments and society as a whole are learning just how vulnerable our businesses and our way of life are to externalities. We are seeing in real time how a shock to individual parts of the system from a natural event have ripple effects across the entire system, be it at the level of an individual business, or at the level of the global economy.
At One Concern, the team has been leveraging and adapting existing epidemiological models to run at hyperlocal scale to enable changed outcomes for public sector and private sector decision makers.
To demonstrate the validity and applicability of this approach, One Concern’s team, led by Dr. Maura Sullivan, conducted an analysis of “The Impact of Hurricane Evacuation on COVID-19 Transmission,” which is included below.
Key findings
- An increased prevalence of infections within a population drastically increases the number of new infections expected within a shelter and can vary vastly depending on the demographic makeup of each specific shelter
- The transmission dynamics and viral characteristics associated with COVID-19 limit the impact and effectiveness of obtaining reliable results from testing especially in time sensitive events like a hurricane evacuation.
- More shelters with smaller capacities are most favorable to reduce the number of new infections within the population housed in shelters
- Length of stay within shelters should be minimized at all cost and is especially critical in large shelters where the potential for transmission is higher
- If possible, elderly individuals or those with pre-existing conditions should be kept out of shelters as they are the most at risk during the pandemic.
- Emergency managers may want to consider an evacuation plan that attempts to keep evacuees from the same geographic area in shelters in order to reduce the potential of exponential spread across a large geographic region
- Those at risk of being impacted by the hurricane, but not in the storm surge zone should be encouraged to practice shelter-in-place. Deciding precisely which areas need to be evacuated and when due to the natural hazard enables waiting as long as safe to start evacuations as minimizing time spent by evacuees in the shelters is critical to reducing infections
- Social distancing and hygiene considerations are important in reducing transmission in shelters, but there is still considerable uncertainty in compliance and enforceability
Hurricanes evacuations result in the movement of populations and close contact between people, which has the potential to significantly exacerbate COVID-19 threat. The COVID-19 pandemic will continue through the 2020 hurricane season and hurricane evacuations coupled with the lifting of shelter in place restrictions have the potential to reseed the pandemic. The 2020 Atlantic hurricane season is predicted to be more active than normal, with a 50% greater than normal probability of a major storm washing the East Coast of the United States. To reduce the impact of hurricane evacuations on pandemic spread, emergency managers can reduce shelter size and length of stay, closely monitor the incidence of potentially infectious cases in the evacuation regions, and utilize non-pharmaceutical interventions, including hand-washing, masks, and social distancing.
Background
The particular viral characteristics associated with COVID-19 makes it a uniquely difficult pathogen to contain. The virus is transmissible in the pre-symptomatic stage, which means that techniques like contract tracing and temperature checks, which were effective in controlling another Coronavirus, SARS, are relatively ineffective in controlling COVID-19. According to one study, almost half of secondary cases were infected during the pre-symptomatic phase and that viral loads, and subsequently infectiousness, likely peak before symptom onset.
Further exacerbating the difficulty of screening for COVID-19 is the high rate of asymptomatic infections. Population estimates from Iceland and Austria indicate that as many as 50% of infections may be asymptomatic or at least subclinical. This is corroborated by a study of the sailors aboard the aircraft carrier, USS Theodore Roosevelt, where 660 of 4,800 sailors tested positive, of which 60% had not shown any symptoms associated with the illness at the time of testing. The asymptomatic rate may vary by demographics, such as age, which may account for some of the discrepancies in estimates. Early prevalence studies out of Stanford, USC, and New York indicate that the actual number of COVID-19 cases may be between 10 and 50 times the official counts.
Hurricanes are rapidly evolving, and response time is critical. This significantly impacts the ability to use testing in order to limit the probability of COVID-19 exposure in shelters and during evacuations. The performance of serologic tests varies greatly and the false negative rate for the rapid Abbot ID NOW test was found to be 15%. Nasopharyngeal swabs are challenging to obtain and testing from the nose only increases the likelihood of a false negative. Additionally, the amount of virus present changes over the course of infection. For COVID-19, the highest viral loads appear to be at the beginning of symptom onset, so if testing occurs too early or too late it is highly probable that the test will miss an infection.
Testing is not likely to be an effective tool for shelter operations. If the prevalence of active COVID-19 is low, false positives are likely to be a major issue. The confirmed COVID-19 case counts for the last two weeks of April in the Miami metro area is ~1 in 1,000 and ~6 in 1,000 in the New York metro area. If a serological test has 90% specificity (probability that a test result is negative when the disease is not present), the positive predictive value will be only 1.7% for Miami and 9.4% for New York. This means that over 90% of positive results will likely be false in New York and over 98% of positive results will likely be false in Miami. Only if a rapid test has over a 99% specificity does the false positive rate become acceptably low to use as a screening tool in large populations for decision-making purposes.
Methodology
One Concern used a compartmental epidemiological model to explore the potential impact of hurricane evacuations on the spread of COVID-19. The model tracks the transition between susceptible, exposed, asymptomatic, presymptomatic, symptomatic (mild and severe), hospitalized, and recovered. We assume that all exposed cases have an incubation period. The model uses a stochastic simulator where the movements between compartments are multinomially distributed based on transition rates. We used the model to explore the impact of shelter size, the population prevalence of infectious cases, length of stay, and transmission reduction measures, including social distancing and masks on infection rates.
In order to determine the range of assumptions for the infection rate prevalence, we reviewed confirmed COVID-19 case counts for the last two weeks of April. Two weeks is likely a conservative estimate of the infectious period, as the average infectious period is assumed to be ~10 days. However, the infectious period does appear to vary based on the severity of the infection and other factors, such as age. One study detected viral particles in one-third of patients for over 20 days after the initial onset of symptoms. However, due to the high rates of subclinical and asymptomatic infection, actual rates are likely much higher than the number of confirmed cases.
In order to quantitatively evaluate the potential impact hurricane evacuation shelters might have on the COVID-19 pandemic, we assume 3 different case rates per 1,000 evacuating residents: 1, 5, and 10. These numbers are consistent with the confirmed COVID-19 case counts for the last two weeks of April in US metro areas and the range of population prevalence rates allows for an exploration of the current uncertainty around the ratio of confirmed cases to asymptomatic and subclinical infections and the possibility that case rates may increase as restrictions are lifted.
We assume 5 different shelter sizes ranging from 25 people to 2,500 people, in accordance with the shelter data from Hurricane Irma. In Lee county, which encompasses Fort Meyers and the surrounding area, 34,000 were in shelters during Hurricane Irma, with shelters housing from 500 to over 6,000 people each. During the peak of Hurricane Irma 191,764 people were housed in shelters. Figure 1, below, is an image from a Florida shelter during the 2017 hurricane season. We assume an average of 3 days were spent in the shelter for our base scenario.
Figure 1: Image Credit: Select Committee on Hurricane Response and Preparedness Final Report January 16, 2018
In our base scenario, we made no changes to shelter operations. As a result of the close contact routinely experienced in shelters each infected individual is assumed to have contact with 50 individuals over the course of a day in a shelter with 2,500 people. Additionally, shelter conditions make it so there is a high possibility of having superspreaders, where one infected individual infects a large number of individuals in a short period of time. Given the transmission dynamics of COVID-19 and the high-levels of mixing in shelters, we assumed homogeneous mixing among the population of an individual shelter.
The epidemiological model was seeded with a minimum of 1 and a maximum of 40 cases for each shelter size, with the exception of the shelter size of 25. The cases entering the shelter were assumed not to be showing any symptoms, as it is expected that the shelters will be doing basic screening for symptoms and quarantining individuals who are ill. The average modeled number of infected and exposed individuals after 3 days in the shelter was used to determine the new cases resulting from each shelter.
We then used binomial probabilities to multiply the modeled average new cases for each run by the probability that each specific number of individuals corresponding to the seed number would enter the shelter. The weighted average of the number of new cases multiplied by the binomial probability was the resulting modeled number of new cases. The results are displayed in new cases per 100,000 people.
Results
With minimal changes to shelter operations and population prevalence of infectious cases consistent with current data, a single hurricane evacuation would be sufficient to significantly exacerbate the pandemic threat and likely reseed the pandemic in the areas that are evacuated. In 2017, three major hurricanes — Harvey, Irma and Maria — displaced over 3 million people in the space of a month. Nearly 7 million Floridians evacuated their homes when Hurricane Irma threatened the region. If we assume the asymptomatic case rate is roughly equivalent to the current confirmed case rate, then a major evacuation with similar sheltering rates as Irma would result in over 12,000 new infections in just the sheltered population at the current population prevalence rate of asymptomatic cases in Miami (1 per 1000) or greater than 50,000 new infections at the current population prevalence rate of asymptomatic cases in New York (6 per 1000). In comparison, Florida is currently reporting 33,000 confirmed cases total since the inception of the pandemic. Each of these new infections has the potential to infect additional people, so in the absence of strict shelter-in-place restrictions COVID-19 would likely spread exponentially in the evacuated communities when the evacuation orders are lifted.
Shelter Size
One factor that could significantly impact transmission dynamics is the size of shelters. If emergency managers are able to reduce the average population of a shelter by avoiding the use of large shelters and instead relying on hotels and other small facilities the number of modeled cases can be drastically reduced. This is a result of both the probability of an infected individual entering a shelter, as well as the number of subsequent individuals each case is likely to infect. At the current presumed infection rates in both Miami and New York there is a greater than 99% chance that at least 1 person will enter a shelter of 2500 people infected with COVID-19. If shelter size is reduced to 25 then there is a less than 12% chance that an infected individual will enter a given shelter. Table 1 illustrates the probability of a single shelter having at least one COVID-19 case by population prevalence of infected cases and shelter size.
Table 1: Probability of a single shelter having at least 1 infected individual
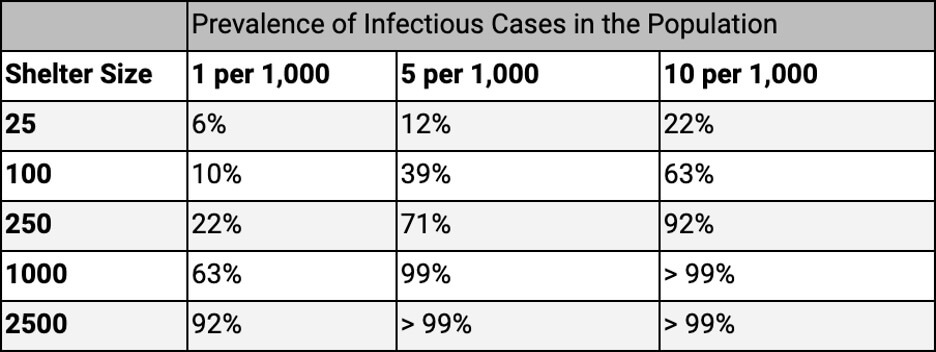
If even a single infected individual is present in a smaller shelter, the models predict a high infection rate within that shelter. This means, if possible, elderly individuals or those with pre-existing conditions should be kept out of shelters entirely as they are the most at risk during the pandemic.
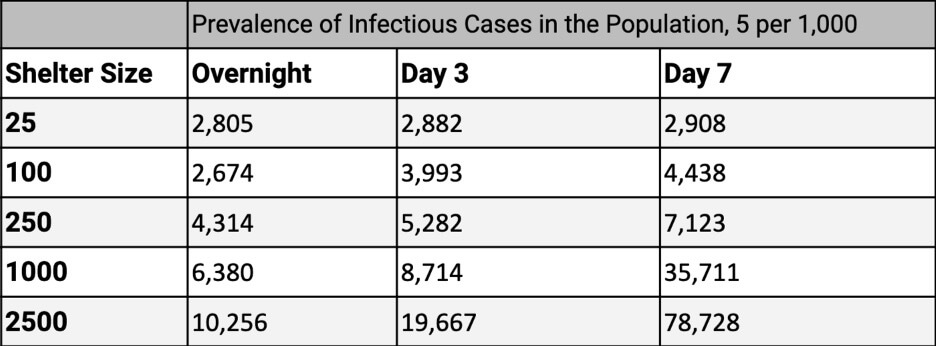
Table 2 illustrates the expected number of new cases per 100,000 evacuees in shelters resulting from 3 days in an evacuation shelter. These results represent the weighted average of the number of new cases from the epidemiological model multiplied by the binomial probability of the number of asymptomatic cases used to seed the epidemiological model. Any evacuation effort is likely to require a combination of shelter sizes and configurations based on available resources, but the relationships can be used to guide decision-making. There is significant variation in case rates between geographic areas, so this underscores the importance of knowing where evacuees are coming from and having up-to-date information on the caseloads and transmission dynamics in the regions that are being evacuated. Our model can use such hyperlocal up-to-date information to tailor the estimates similar to how our flood inundation map provides hyperlocal predictions and updates with hyperlocal up-to-date information from stream gauges, etc. Emergency managers can use both information about the hazard and people impact to make tailored decisions for each region.
For example, emergency managers may want to consider an evacuation plan that attempts to keep evacuees from the same geographic area in shelters in order to reduce the potential of exponential spread across a large geographic region and assist with contract tracing once the evacuation orders are lifted.
Table 2: Expected number of new cases per 100,000 evacuees in shelters after 3 days in an evacuation shelter

Shelter Stay Length
Minimizing the length of shelter stay is an important way to reduce the number of shelter-acquired infections. The transmission of respiratory infections is increased when populations are living in close quarters. The 1918 influenza pandemic is thought to have taken hold in a military camp in Kansas, where close quarters facilitated disease transmission. Hospital-acquired infections have been shown to increase with length of stay. Even if larger shelters are required initially, moving evacuees to smaller shelters as soon as possible will help limit the spread. The model assumes a homogenous mixing rate in the shelter population, so each person is equally likely to encounter any other person. This results in an overestimation of case rates for the largest shelter size as the number of days increase, because people tend to interact with the same people repeatedly.
Table 3: The expected number of new cases per 100,000 evacuees in shelters after 3 days in an evacuation shelter with the enforcement of social distancing and hygiene measures
COVID-19 changes the risk equation, so that the risk of illness must be weighed against natural catastrophe and evacuation risk. Those at risk of being impacted by the hurricane, but not in the storm surge zone should be encouraged to practice shelter-in-place. Deciding precisely which areas need to be evacuated and when due to the natural hazard enables waiting as long as safe to start evacuations as minimizing time spent by evacuees in the shelters is critical to reducing infections.
In-Shelter Interventions
If evacuation shelters are required, social distancing and hygiene measures must be implemented to control spread, especially in larger shelters. We explored the impact of non-pharmaceutical interventions designed to reduce the number of contacts and the probability of infection given contact in the shelter scenario. We evaluated 3 social distancing scenarios and 3 hygiene scenarios. The social distancing scenarios model the impact of measures designed to reduce the contact rate between individuals and the hygiene scenarios include personal protection measures, such as masks and hand-washing, designed to reduce the probability of transmission when contact does occur.
The model contains the following social distancing measures:
- No social distancing: 100% of the baseline contact rate: No changes to typical shelter operations.
- Moderate social distancing: 60% of the baseline contact rate: Individuals would be required to maintain a distance of 6 feet to the fullest extent possible with anyone outside their household. Significant changes to shelter density, sleeping arrangements, meal distribution, and logistical operations would be required.
- Extreme social distancing: 20% of the baseline contact rate: Movement in the shelter would be severely restricted and individuals would be required to interact only with their household. Sanitary barriers would be erected throughout the shelter providing a physical barrier between household groups. Bathroom use would be restricted in order to maintain safe distancing and meals would be distributed individually by workers wearing personal protective equipment (PPE).
Personal hygiene measures including coughing etiquette, meticulous hand washing, and avoiding touching the face have been shown to reduce the probability of transmission for respiratory viruses. However, these measures are difficult to enforce, especially in living and sleeping quarters. There is conflicting evidence supporting the use of non-medical grade face masks in preventing transmission of respiratory illness in communities. They may serve to reduce the probability of transmission by minimizing the number of respiratory droplets excreted by infected individuals. One recent study shows that a review of all available evidence suggests that near-universal adoption and compliance of non-medical masks when in public combined with other public health measures could stop community spread of COVID-19. However, near-perfect compliance in a shelter situation is not possible, as it is not possible to enforce compliance during sleep and within population groups such as young children who typically have low rates of compliance.
For this reason the potential impact of social distancing measures is greater than the impact of personal hygiene measures. The model contains the following hygiene measures:
- No change to personal hygiene: 100% of the baseline transmission rate: No changes to typical shelter operations.
- Moderate personal hygiene: 75% of the baseline transmission rate: Individuals would be required to wear cloth face coverings or surgical masks as available. Hand sanitizer and hand-washing stations would be placed throughout the facility. Individuals with respiratory excretions for any reason, including not related to disease, would be separated from the general population.
- Extreme personal hygiene: 50% of the baseline transmission rate: Surgical masks would be required and new masks would be provided daily. Individuals would be required to wear gloves when leaving personal areas.
Table 4: The expected number of new cases per 100,000 evacuees in shelters after 3 days in an evacuation shelter with the enforcement of social distancing and hygiene measures*
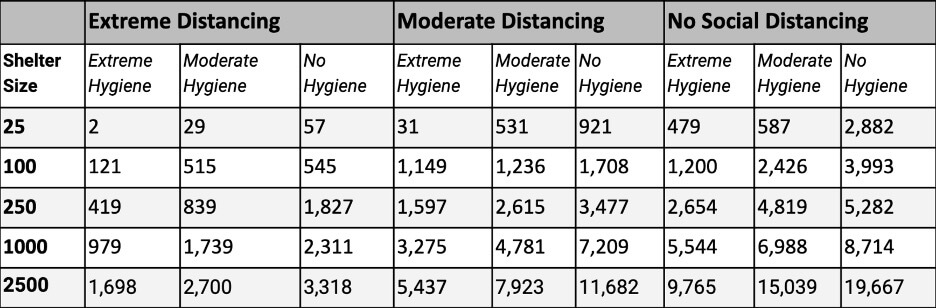
* Prevalence of Infectious Cases in the Population, 5 per 1,000
There is a point at which adding additional social distancing or hygiene measures is likely not worth the cost and effort, especially in smaller shelters. Due to the stochastic nature of the model the results become somewhat unstable for very low values and the uncertainty bounds likely include 0 cases. The impacts for small shelters and extreme distancing and hygiene should be interpreted as directional, rather than absolute values. The model contains a limited number of buckets of contact rate and transmission rate representing social distancing and hygiene. However, in reality there are an infinite number of combinations related to the selection of measures, compliance of the population, and efficacy of the measures. The efficacy of different social distancing and hygiene measures is a subject of ongoing research and as we learn more about the transmission dynamics of COVID-19, modeling assumptions can be refined to better assist decision-makers.
Discussion
There is significant uncertainty around the SARS-CoV-2 and COVID-19, the disease that it causes. Despite the feverish pace of research, there will continue to be uncertainty around factors including transmission dynamics, fatality rate, population prevalence, the asymptomatic infection rate, and the impact of interventions. Despite the high-level of uncertainty, decision-makers are going to have to decide when and how best to engage in necessary emergency activities, like hurricane evacuations, and other non-emergency activities that have a similar decision criteria.
This model could be extended to assist with understanding the risk of infection for opening schools, workplaces, or other places where people gather. By utilizing hyper-local data around infections rates, One Concern can assess the hazard associated with the spread of infectious diseases across populations, spanning from small groups like the employees of a company entering and exiting a building daily, to large groups of residents within a county. One Concern uses real-time data ingestion to better inform models across hazards and combines these outputs at a hyper-local level. Most importantly, understanding what can happen if there are multiple disasters which happen at the same time such as a hurricane and subsequent evacuation during a pandemic, is key to helping decision-makers better change outcomes.
About One Concern
At One Concern, we are a climate resilience technology company dedicated to empowering organizations with actionable insights to address the impacts of business disruption caused by disasters. Through our analytics, we enable risk selection, mitigation, pricing, scenario analysis, and risk management. Our mission is to make disasters less disastrous by helping organizations understand and prepare for downtime from physical climate risks. We are committed to providing the world with the tools needed to effectively mitigate and manage downtime from such risks. Learn more about us at oneconcern.com.